
Dental Implant Training for General Dentists: What to Know Before You Start | WSS
dental implant training for general dentists

Dental implants represent one of the most significant expansions a general dentist can make to their clinical scope. The procedures are predictable, the outcomes are excellent when performed correctly, and patient demand for implant-retained restorations continues to grow year over year.
Yet most general dentists still refer implant cases to oral surgeons or periodontists — not because the procedures are beyond their clinical reach, but because the training pathway feels unclear. This article addresses that directly: what dental implant training actually involves, what skills it builds, how it connects to surgical training you may already be pursuing, and what to look for when evaluating CE programs.
Whether you are just beginning to consider implant placement or are actively researching programs, this guide provides the foundation you need to make a well-informed decision.
Why General Dentists Are Well-Positioned for Implant Placement
The case for general dentist implant placement is grounded in both clinical reality and scope of practice. General dentists routinely manage alveolar bone, soft tissue, and osseointegration contexts — through extractions, socket preservation, and surgical placement procedures that are closely related to implant surgery.
The skills that make a general dentist competent in oral surgery translate directly to implant placement: the ability to assess bone volume and quality on imaging, manage a surgical field, make incisions and manage flap design, and execute a planned procedure with precision under clinical conditions.
What distinguishes implant placement from routine surgical extraction is the prosthetic planning dimension. Implant placement requires understanding not just the surgical site, but the final restoration — where the implant needs to be positioned to support the crown, how bone remodeling will affect the gingival contour, and how prosthetic components will load the implant over time. This dimensional thinking is what training programs must build, alongside the surgical technique itself.
Implant placement is not a fundamentally different clinical domain from the surgical work general dentists already do. It is an extension of the same skill set, applied with a restorative endpoint in mind.
The Core Skills Dental Implant Training Develops
A well-designed implant training program builds competency in six core areas. Understanding what these are helps you evaluate whether a program you are considering actually addresses them.
1. Treatment planning and case selection
Successful implant outcomes begin with appropriate case selection. Treatment planning for implants involves radiographic assessment — typically including CBCT imaging to evaluate bone volume, density, and proximity to anatomical structures — and clinical evaluation of tissue quality, occlusal loading factors, and systemic health considerations. Training programs should develop a systematic approach to this assessment that can be applied consistently across patient types.
2. Surgical site preparation
Before an implant can be placed, the site must be prepared to receive it. This includes extraction of the failing tooth if still present, socket preservation with bone grafting material if necessary, and soft tissue management that will support long-term esthetic outcomes. These procedures are often performed in a staged sequence, and training should address both the individual procedures and the sequencing logic that determines which to perform and when.
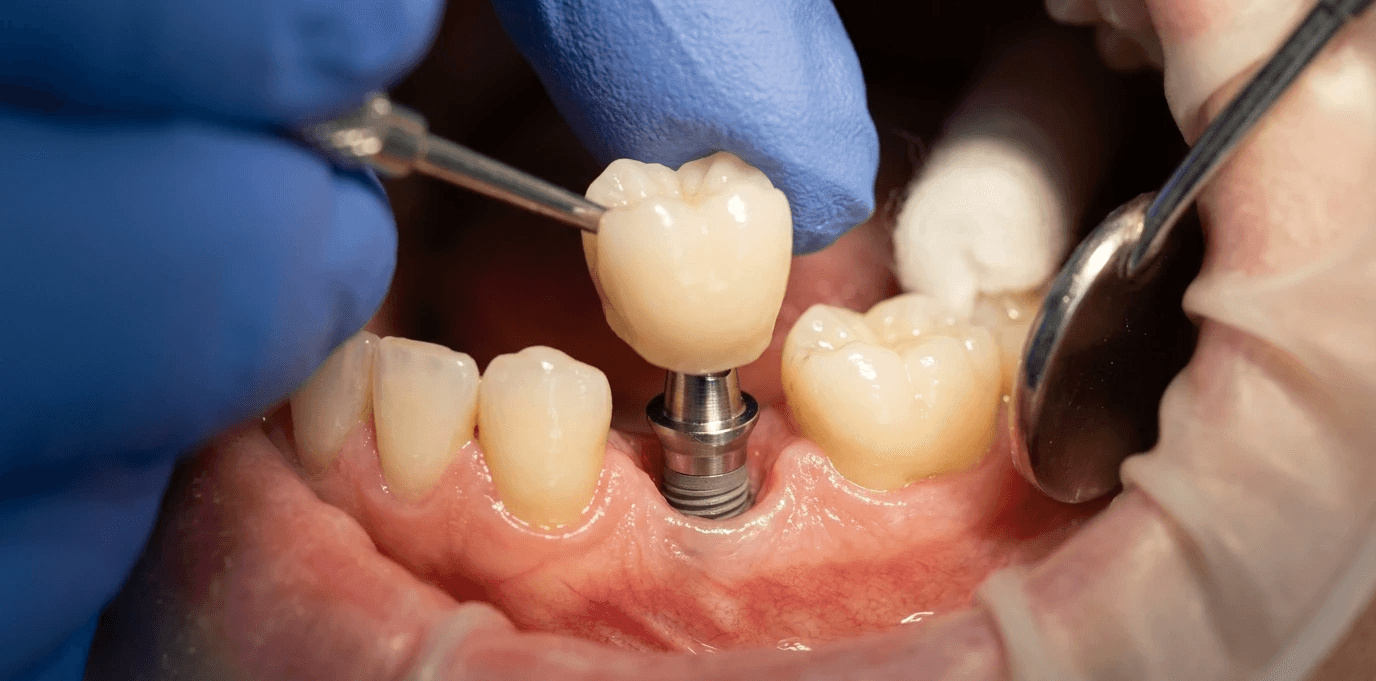
3. Implant placement technique
The placement procedure itself involves implant site preparation with sequential drills, implant seating at the correct depth and angulation, and primary stability assessment. Guided implant surgery — using 3D-printed surgical guides derived from CBCT planning — is now widely used and significantly improves placement accuracy, particularly for less experienced surgeons. Training programs should include both freehand and guided placement approaches.
4. Prosthetic integration
Understanding the relationship between surgical placement and prosthetic design is what separates a well-trained implant surgeon from one who places implants in the wrong position. Training should develop the ability to work backwards from the planned restoration — using diagnostic wax-ups, digital planning, or surgical guides — to ensure that placement decisions support the final prosthetic outcome.
5. Complication recognition and management
Implant complications range from minor soft tissue problems to significant osseointegration failures. Training programs should cover the recognition, management, and prevention of the most common complications, including implant failure, peri-implantitis, nerve proximity errors, and sinus involvement in posterior maxillary cases.
6. Patient communication and consent
Implant patients require thorough informed consent that covers the multi-stage nature of treatment, the realistic timeline to final restoration, the possibility of bone grafting, and the risk of implant failure. Training should develop the ability to communicate this clearly and manage patient expectations throughout a treatment sequence that may span six to twelve months.
How Implant Training Connects to Surgical Training
Dentists who have completed training in surgical extraction — particularly impacted third molar extractions — are better prepared for implant training than dentists who have not. The overlap is significant and intentional.
Surgical extraction training builds the manual dexterity, tissue management instincts, and clinical decision-making reflexes that implant placement requires. A dentist who has performed 50 impacted third molar extractions under supervision has developed a working relationship with the surgical field, flap design, and handpiece technique that directly transfers to implant surgery.
This is why the progression from surgical extraction training to implant training is logical rather than arbitrary. It reflects the actual clinical skill hierarchy — not simply a course catalog sequence.
Western Surgical and Sedation's Impact7 surgical training program is designed with this progression in mind. Dentists who complete the Impact7 curriculum develop foundational surgical competency that prepares them for the next stage of clinical expansion, whether that involves implant training, advanced bone grafting, or other surgical procedures.
The most efficient path to implant competency runs through surgical extraction training first. Dentists who develop their hands on extraction cases build the clinical foundation that makes implant training faster, more effective, and more confidence-building.
What to Look for in a Dental Implant CE Program
The dental implant CE landscape is extensive, and the quality of available programs varies significantly. These criteria help separate programs that build genuine clinical competency from those that deliver theoretical familiarity.
Live patient surgery, not just typodont practice
Placing implants on a typodont in a lab setting is useful for learning drill sequences and basic orientation, but it does not replicate the clinical variability of a real surgical site. Blood, tissue response, bone density variation, and patient movement are all factors that only live patient training addresses. A program that offers typodont practice only is not preparing you for the operatory.
CBCT planning integration
Implant training that does not incorporate CBCT-based planning and guided surgery is teaching outdated technique. Modern implant placement is built around three-dimensional imaging and surgical guides that dramatically improve accuracy and safety. Your training should include hands-on experience with planning software and surgical guide fabrication or use.
Restorative faculty involvement
Because implant placement is inseparable from prosthetic design, programs that include both surgical and restorative faculty provide a more complete education than those that address only the surgical component. Understanding how your restorative colleague will build the crown on the implant you place changes how you plan and execute the surgical procedure.
Mentorship after the course
Post-course mentorship is as important in implant training as in surgical extraction training. Your first solo implant case will raise questions that your training prepared you to recognize but that benefit from a more experienced voice. Programs that provide ongoing case consultation and faculty access after training ends produce better clinical outcomes and more confident practitioners.
Frequently Asked Questions
Do I need to complete surgical extraction training before implant training?
It is not a formal requirement, but it is strongly recommended. Dentists who attempt implant training without a foundation in surgical technique often find the learning curve steeper and the transition to solo cases slower. Completing surgical extraction training first builds the manual skills that make implant training more efficient and more effective.
What equipment do I need to add to my practice for implant placement?
Core additions include a surgical handpiece compatible with implant drill kits, CBCT imaging capability or a referral relationship with an imaging center, a surgical kit for the implant system you choose, and bone graft materials. The specific requirements depend on the implant system and case types you plan to offer. Your training program should provide a detailed equipment list specific to the system taught.
How many implants should I place before considering myself competent?
Competency development in implant placement follows a curve rather than a threshold. Most training programs target 20 to 30 supervised placements as the foundation for solo practice, with the understanding that competency continues to develop with each subsequent case. Starting with appropriately selected cases — adequate bone volume, favorable anatomy, single tooth restorations — and expanding case complexity as experience accumulates is the standard approach.
Will my malpractice insurance cover implant placement?
Most general dentist malpractice policies cover implant placement; confirm with your carrier before your first case. Documentation of your training and any CE certificates should be kept on file as evidence of competency development.
Build the surgical foundation first.
The Impact7 Techniques Course gives general dentists the live patient surgical training that prepares them for implant placement and beyond. Start where the skill progression begins.
Explore Impact7 at westernsurgicalandsedation.com/courses




Related Articles
Related reading
Explore articles connected to surgical training, IV moderate sedation, and real world clinical decision making, selected to support dentists applying advanced care in daily practice.


