

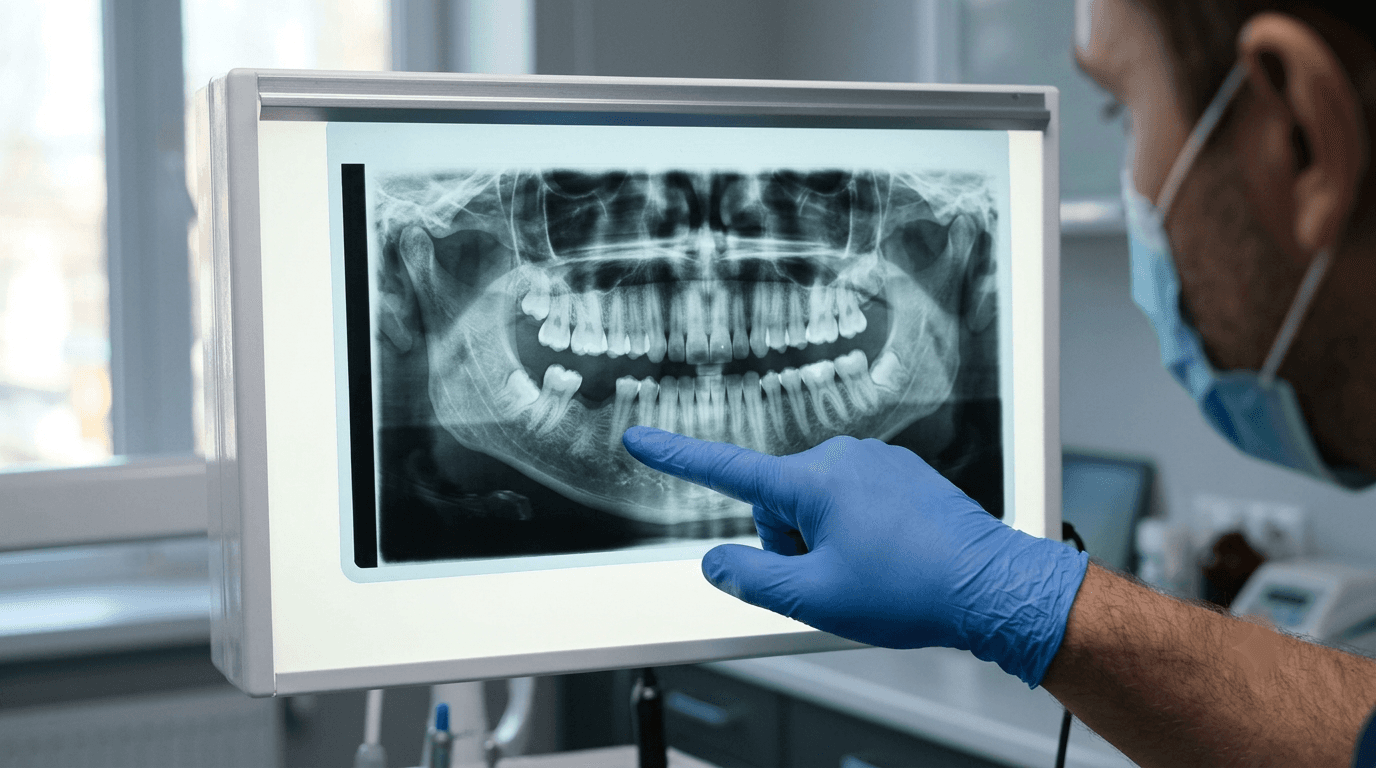
Every tooth extraction sets off a predictable biological process: the alveolar bone that once surrounded the root begins to resorb. Within six months of an unpreserved extraction, a patient can lose up to 50 percent of the ridge width and a significant portion of ridge height. For a patient who may want an implant in that site someday, this resorption can mean the difference between a straightforward implant placement and a case requiring extensive bone grafting before placement is even possible.
Socket preservation — placing bone graft material into an extraction site at the time of extraction — is one of the most valuable, and most underutilized, procedures in general dental practice. It is technically straightforward, adds meaningful revenue to an extraction appointment, and protects the patient's future treatment options in a way that costs far less than reconstructive grafting later.
This article covers what socket preservation and bone grafting actually involve, why they matter clinically, and how general dentists can build this skill as a natural extension of surgical extraction training.
Why Extraction Sockets Resorb — and Why It Matters
The alveolar bone that surrounds a tooth root exists because the tooth is there. Once the tooth is removed, the biological signal that maintained that bone is gone, and the body begins remodeling the site. This is not a pathological process — it is the expected physiological response to extraction.
The consequence for future treatment planning is significant. Reduced ridge width and height can compromise the site's ability to support an implant without additional grafting. For patients who are uncertain about future implant treatment, or who cannot afford it immediately after extraction, an unpreserved socket can close the door on straightforward implant placement by the time they are ready.
Socket preservation interrupts this resorption process by filling the extraction site with graft material and often a barrier membrane, maintaining ridge dimensions closer to their pre-extraction state and keeping future treatment options open.
A socket that is preserved at the time of extraction is a socket that stays implant-ready. A socket that is not preserved often requires a separate, more invasive grafting procedure before an implant can be placed at all.
What Socket Preservation Actually Involves
The procedure is performed immediately following extraction, while the surgical site is already open and accessible. This is one of its key advantages — it adds relatively little additional chair time to a procedure the patient is already having.
Step 1: Atraumatic extraction
Socket preservation begins with the extraction itself. Minimizing trauma to the surrounding bone and soft tissue during extraction preserves more of the native anatomy for the graft to work with. This is another area where surgical technique developed through structured extraction training directly benefits outcomes.
Step 2: Socket debridement
The socket is thoroughly curetted to remove any remaining periodontal ligament tissue, granulation tissue, or infection. A clean socket is essential for predictable graft incorporation.
Step 3: Graft material placement
Bone graft material — which may be allograft (donor bone), xenograft (bovine-derived), synthetic, or a combination — is packed into the socket to fill the space left by the root. The choice of graft material affects resorption rate, cost, and handling characteristics, and is typically guided by the specific clinical situation and the practitioner's training.
Step 4: Membrane placement (when indicated)
A resorbable collagen membrane is often placed over the graft material to prevent soft tissue from growing into the socket before bone can form. This barrier function is particularly important in sites where the buccal bone plate has been compromised.
Step 5: Soft tissue management and closure
Depending on the socket and the amount of soft tissue available, the site may be closed with sutures, covered with a collagen plug, or left to heal with the membrane exposed. This decision depends on case specifics that training should address directly.
When Socket Preservation Is Indicated
Socket preservation is not necessary for every extraction, but it is strongly indicated in several common clinical scenarios:
Any site where future implant placement is being considered, even if the timeline is uncertain
Anterior extractions where esthetic ridge contour is a priority for future restoration
Sites with thin buccal bone plates, which are at higher risk of significant resorption
Molar extractions where the socket is large and would otherwise heal with substantial bone loss
Patients who are young and likely to need implant restoration decades in the future, where preserving options matters most
Conversely, sites being restored with a fixed bridge or removable prosthesis, and sites where the patient has explicitly decided against future implant treatment, may not require preservation — though the decision should always be discussed directly with the patient given the uncertainty most people have about their future treatment preferences.
The Case for Adding Socket Preservation to Your Extraction Practice
For general dentists who have already developed surgical extraction competency — through training such as the Impact7 Techniques Course — socket preservation is a natural next step that requires relatively modest additional training investment.
Clinical rationale
If you are already performing the extraction, the incremental time and skill required to preserve the socket is small relative to the extraction itself. The socket is open, the patient is already anesthetized, and the additional procedure typically adds 10 to 15 minutes to the appointment.
Revenue rationale
Socket preservation is billed separately from the extraction itself, typically in the range of $300 to $600 per site depending on the graft material used and geographic market. For a practice performing multiple extractions weekly, this represents a meaningful revenue addition with minimal additional chair time.
Patient value rationale
Beyond the direct revenue, socket preservation protects your patient's future treatment options and reduces the likelihood that a delayed implant decision requires an additional, more expensive bone grafting procedure. This is a genuine clinical benefit that is straightforward to communicate to patients during the informed consent conversation for extraction.
How Socket Preservation Connects to Implant Training
Dentists who are considering implant placement training benefit significantly from developing socket preservation skills first, or concurrently. The two procedures share overlapping clinical judgment: assessing bone quality, understanding graft material handling, and anticipating how a site will heal and what it will support.
A dentist who has preserved 30 or 40 extraction sockets has direct, hands-on familiarity with bone graft materials, healing patterns, and the relationship between socket management and eventual implant readiness — familiarity that translates directly into more confident implant case planning.
This progression — extraction training, then socket preservation, then implant placement — reflects a logical skill-building sequence rather than an arbitrary course catalog. Each stage builds directly on the clinical judgment developed in the prior stage.
What to Look for in Bone Grafting Training
As with any surgical skill, the quality of training determines whether you develop genuine clinical competency or simply theoretical familiarity.
Hands-on graft placement, not just lecture content
Understanding graft material properties from a lecture is useful, but developing the tactile sense of proper graft compaction, appropriate membrane adaptation, and suture technique for socket closure requires hands-on practice, ideally on live patients under supervision.
Exposure to multiple graft material types
Different clinical situations call for different graft materials. Training that only covers a single product line limits your ability to make material selection decisions based on the clinical situation rather than habit.
Integration with surgical extraction training
Programs that teach socket preservation as an integrated component of surgical extraction training — rather than as an entirely separate course — provide a more coherent learning experience and reflect how these skills are actually applied in practice.
Frequently Asked Questions
Does socket preservation guarantee successful future implant placement?
Socket preservation significantly improves the likelihood of straightforward implant placement by maintaining ridge dimensions, but it does not eliminate all future grafting needs in every case. Some sites, particularly those with significant pre-existing bone loss from periodontal disease, may still require additional grafting at the time of implant placement even after socket preservation.
How long after socket preservation can an implant be placed?
Typical healing time before implant placement in a preserved socket is 4 to 6 months, allowing adequate bone formation and maturation. This timeline can vary based on graft material used and individual healing response, and should be confirmed radiographically before proceeding to implant placement.
Is socket preservation necessary for every extraction site?
No. Sites that will be restored with options other than an implant, or where the patient has clearly decided against future implant treatment, may not require preservation. However, given the uncertainty most patients have about future treatment decisions years in advance, many practitioners recommend preservation as a default unless there is a specific reason not to.
What if I extract a tooth and don't preserve the socket, but the patient wants an implant later?
Implant placement is still possible in a resorbed site, but it typically requires a separate ridge augmentation or bone grafting procedure prior to implant placement — adding cost, time, and an additional surgical procedure that socket preservation at the time of extraction would have avoided.
Build the complete surgical skill set — not just the extraction.
The Impact7 curriculum develops surgical extraction technique alongside the site management skills — including socket preservation — that protect your patients' future treatment options.
Explore the curriculum at westernsurgicalandsedation.com/courses




Related Articles
Related reading
Explore articles connected to surgical training, IV moderate sedation, and real world clinical decision making, selected to support dentists applying advanced care in daily practice.


